Smith in 1849 first attempted tubal catheterization (TC) using a whalebone. In 1985, Platia and Krudy described transvaginal TC at the time of laparoscopy. Confino and others described the currently used X-ray-guided technique for TC in 1986.
Here are some images from an actual case study.

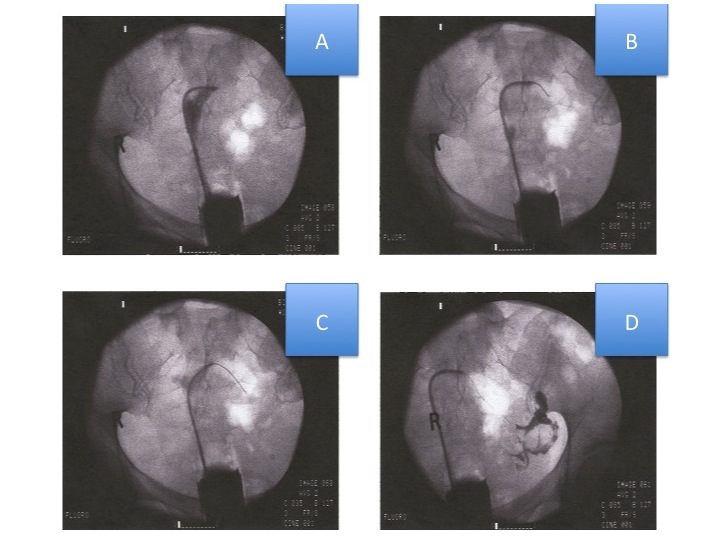
A HSG confirmed the presence of bilateral proximal tubal occlusion (PTO). A decision was made to proceed with TC. As shown above
A selective salpingography (SS) catheter has been manipulated into the left tubal ostia (opening). There is back flow of dye back into the uterine cavity and the tube remains blocked.
A wire guide has been inserted through the central lumen of the SS catheter past the occluded portion into the distal tubal lumen.
The wire guide is now being moved in a to and fro manner to further open up the tube.
Subsequent instillation of dye shows the left tube to be open. The tube has a normal contour (shape) and there is free spill of dye.
The same procedure was then repeated on the other side. The entire process took about five minutes to complete.
TC is successful in 70 – 92% of patients. It is possible to open at least one tube in 90% and both tubes in 80% of patients. In 68% of patients, the tubes remain open at 6 months after the procedure. Spontaneous pregnancy rates after TC approach 40% in patients where the tubes are otherwise normal (no distal tubal disease). This is comparable to what is achieved after complicated and expensive microsurgery.
In patients with normal fallopian tubes following recanalization, the tubal pregnancy rate is similar to that of the normal population. In patients with other factors e.g scar tissue (peritubal adhesions) the rate approximates 3%
The amount of radiation to the ovaries approximates 1 rad (10 mGy), a dose that is within acceptable limits for women of reproductive age. There is small risk of making a hole in the tube with a wire guide. These heal spontaneously and do not require any active management. There is potential for infection associated with a vaginal procedure. We therefore routinely give patients a prophylactic antibiotic (Z-Pak or Doxycycline).

Dr. Karande is Board Certified in the specialty of Obstetrics and Gynecology as well as the subspecialty of Reproductive Endocrinology and Infertility. He is a Fellow of the American College of Obstetricians and Gynecologists and Member of the American Society for Reproductive Medicine.
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists


Comments