Most IVF cycles fail after embryo transfer when the embryo fails to implant. The three factors that can cause implantation failure are:
Several studies have looked at various medical approaches to improve implantation. One such approach that has shown to improve implantation is a physical scratch on the endometrium in the cycle preceding IVF -- “endometrial scratch ”, or ES. We'll look at what ES is, how it's performed, and evidence about its effectiveness in this post.
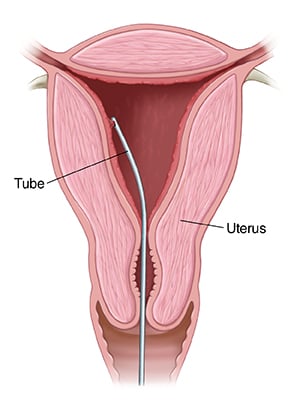 This is a simple procedure that involves using a small catheter or tube with a plunger (which causes suction when it is pulled out). The catheter is introduced through the opening of the uterus (cervix) and a small piece of the endometrium is sampled. It takes a couple of minutes to do the procedure and patients may experience some cramping during and/or after.
This is a simple procedure that involves using a small catheter or tube with a plunger (which causes suction when it is pulled out). The catheter is introduced through the opening of the uterus (cervix) and a small piece of the endometrium is sampled. It takes a couple of minutes to do the procedure and patients may experience some cramping during and/or after.
We do not know for sure. Several mechanisms have been suggested.
A recent survey done in Europe and New Zealand showed that almost 80% of clinics are offering ES to their patients. Data for its use in the US are not available.
Several studies have shown improved implantation rates when ES was done in patients who had failed several IVF cycles. However, is ES effective in patients undergoing their first or second IVF cycle?
This very question was addressed by Frantz et al. from Bordeaux, France in a randomized controlled multi-center, two-arm, parallel trial published in a recent issue of the journal Human Reproduction (Vol. 34, No.1 pp. 92-99, 2019). The study was started in February 2010 and stopped prematurely in July 2014 after an unplanned interim analysis. At the time of study closure, 191 of the planned 358 patients had been included.
Patients included in the study were randomly assigned to either the ES arm or the non-ES arm. Local ES was performed between Day 20 and Day 24 of the cycle preceding ovarian stimulation using a device for endometrial biopsy. Ovarian stimulation used a combination of recombinant FSH and either an GnRH agonist protocol or a GnRH antagonist protocol without any estrogen pre-treatment.
Clinical pregnancy rate (CPR) was analyzed on an intent-to-treat basis. All comparisons between the two groups were done using a logistic regression model adjusted for age, BMI and infertility etiology.
Sixty-eight embryo transfers were performed in the ES arm and sixty-four in the non- ES arm. CPR was 23.5% (16/68) in the ES arm and 35.9% (23/64) in the non-ES arm (hazard ratio (HR) = 0.43; 95% CI, 0.18–1.02; P = 0.0568). The implantation rate was 19.1% and 24.0% in the ES arm and in the non-ES arm, respectively. Two miscarriages and one ectopic pregnancy were reported in each arm.
The multiple pregnancy rate was higher in the scratch arm (50.0% vs 20.0%), but the difference was not statistically significant (odds ratio (OR) = 4.54; 95% CI, 0.50–40.93; P = 0.1349). The endometrial biopsy procedure was well tolerated in most women. Of 50 patients in the ES arm having received the embryo transfer, 40 (80.0%) patients reported having felt pain during the procedure, the pain resolving quickly for 31 of them.
The patients that had ES had a lower pregnancy rate than those that did not. In fact, they looked at this and stopped the study halfway! ES should not be offered to patients undergoing their first or second IVF attempt.
Mak et al. conducted a RCT to assess the impact of ES in women using frozen embryos and found no difference in clinical pregnancy and implantation rates between the ES group and the non-ES group (Reprod Biomed Online 2017;35:28-36).
Karimzade et al. reported that performing ES in the transfer cycle on the day of oocyte retrieval had detrimental effects (Arch Gynecol Obstet 2010;281:499-503).
We do not recommend ES routinely to our patients at InVia. We have done a few in patients that have failed several cycles. Our current approach to patients with implantation failure will be discussed in a future blog.
If you have questions about your fertility and want to work with a board-certified fertility specialist, we can help. We have four convenient locations in the Northwest and North suburbs of Chicago. Please call 847-884-8884 to schedule an appointment. You can also schedule an appointment online using the link below. We are here to serve you and help you achieve your dream of having a baby.


Dr. Karande is Board Certified in the specialty of Obstetrics and Gynecology as well as the subspecialty of Reproductive Endocrinology and Infertility. He is a Fellow of the American College of Obstetricians and Gynecologists and Member of the American Society for Reproductive Medicine.
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists


Comments