
.jpg?width=300&name=My%20project-1%20(37).jpg) When a diagnosis of recurrent pregnancy loss (RPL) is reached after multiple miscarriages, there are many things to consider, including the causes, tests, and common treatments of RPL.
When a diagnosis of recurrent pregnancy loss (RPL) is reached after multiple miscarriages, there are many things to consider, including the causes, tests, and common treatments of RPL.
In this blog, we will discuss five commonly asked questions regarding RPL, including how it is diagnosed and defined as well whether for chromosomal abnormalities, and common causes of RPL. Much of the information here is based on data published by Dr W.H. Kutteh at Vanderbilt University Medical Center.
RPL occurs in at least 1.3% of pregnancies. If two miscarriages are the defining number, the theoretical incidence of RPL is 1 in 45 women. If four miscarriages are used to define RPL, the incidence is 1 in 2,000. If six miscarriages are used to define RPL, the incidence is 1 in 90,000.
The mother’s age also plays a big role in the incidence of miscarriages. At age 20, the incidence of RPL is 1 in 85, by age 30 it is 1 in 45 women and by age 40 it increases to 1 in 4 women. This is usually related to the increase in chromosomal abnormalities (aneuploidy) as a woman ages. The risk of having an aneuploid egg is 10% at age less than 35 y, 30% at age 40 y, 50% at age 43 and 100% at age 45 y.
The number of multiple miscarriages used to define RPL can vary: Traditionally, RPL was defined as three or more spontaneous consecutive pregnancy losses, and in some cases also included a statement that the same partner fathered them. In 2012, the American Society for Reproductive Medicine Practice Committee issued a statement that defined RPL “as a disease distinct from infertility defined by two or more failed consecutive pregnancies." Most insurance companies will agree to pay for complete evaluation for RPL after two consecutive losses.
Certainly, the definition of a pregnancy will affect the definition of a pregnancy loss. There is a spectrum for pregnancy loss based on gestational age (pregnancy of unknown location (PUL), early embryonic loss (less than 6 weeks), embryonic loss (6 – 9 weeks), fetal loss (9 – 20 weeks), miscarriage (less than 20 weeks) and stillbirth (greater than 20 weeks)).
The traditional definition of a pregnancy loss came from the textbook Williams Obstetrics, which stated that “a miscarriage is the loss of a pregnancy before 20 weeks of gestation or less than 500 grams.” This definition made diagnosis of a pregnancy loss very easy; any woman who had a confirmed pregnancy that failed was categorized as having a miscarriage.
To define pregnancy loss, the American Society for Reproductive Medicine (ASRM) Practice Committee first defined pregnancy in aPractice Bulletin “as a clinical pregnancy documented by ultrasonography or histopathologic examination.” This has added some confusion to the field in that a pregnancy that is lost without an ultrasound being performed or without the products of conception being evaluated does not “count” as a miscarriage. It further does not consider those well-documented pregnancies that are termed “biochemical losses.”
The Royal College of Obstetrics and Gynecology defined miscarriage as “a spontaneous loss of pregnancy before the fetus reaches viability.” Their guideline states “all pregnancies losses from the time of conception until 24 weeks of gestation should be included.” This more inclusive definition seems more practical based on clinical experience. Certainly, many patients consider a miscarriage any pregnancy in which they have had a positive pregnancy test that does not result in the birth of baby.
At InVia Fertility Specialists, we consider pregnancy loss as a pregnancy that is documented by an appropriately rising quantitative hCG that ultimately fails.
Yes, both parents should be checked.
It is often argued that genetic testing on the parents is not necessary because: (1) the frequency of genetic abnormalities in the parents from couples with RPL is only 3 to 5% and (2) genetic testing with karyotype analysis is expensive. Conventional karyotypes cost approximately $850 each with 23-chromosome microarray being more expensive. The prices, however, are coming down as these tests are being used more frequently
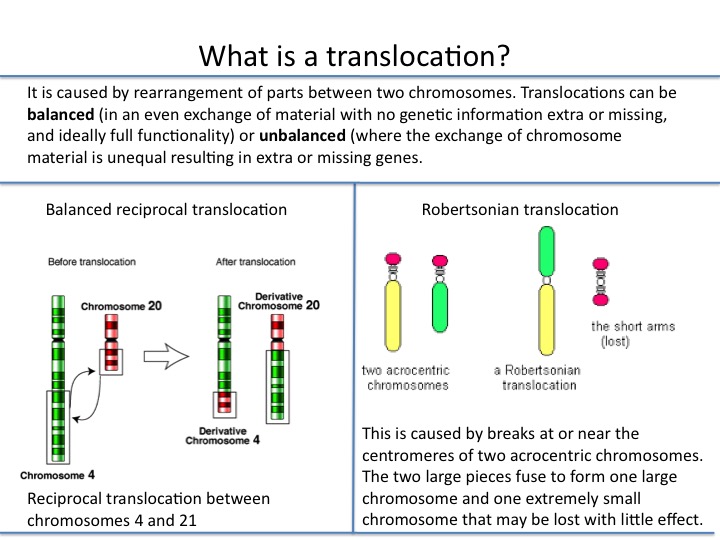
However, in couples with RPL who have a parental genetic abnormality, a balanced translocation is the genetic abnormality in 85% of cases. These include both reciprocal translocations (59%) and Robertsonian translocations (27%). Inversions (9%), sex chromosome aneuploidies (4%), and supernumerary chromosomes (1%) are detected less frequently. The importance of obtaining karyotypes on the parents should not be minimized. The karyotype results from the parents can provide prognostic information for subsequent pregnancies.
For example, if the parent has a reciprocal translocation, the chance of a subsequent miscarriage is 50 to 70%. If one the parent harbors a Robertsonian translocation, the chance for a subsequent miscarriage is 30 to 50% with the exception being if the translocation is to the same chromosome. Similarly, inversions in parental chromosomes results in subsequent miscarriages of at least 30%
Studies on preimplantation embryos from women with RPL undergoing in vitro fertilization provide interesting data when compared with the genetic abnormalities found in the miscarriage tissue. The possibility exists that certain aneuploidies and other abnormalities that are detected in miscarriage tissue from women with RPL represent those abnormalities that restricted the pregnancy grow up to a certain point. The most common chromosomal abnormalities seen in products of conception include those from chromosome 16, 22, 21, and 15. These account for almost 60% of all genetic results. Conversely, aneuploidies in chromosome 1 are rarely seen in products of conception, whereas those from chromosomes 2 through 7 are seen less than 10% of the time.
Recent data from preimplantation genetic screening on more than 2,000 embryos from RPL patients who underwent in vitro fertilization indicate that aneuploidy in the developing embryo exists at significant rates in all 23 pairs of chromosomes when evaluated both at the cleavage stage and the blastocysts stage, as identified by microarray preimplantation genetic screening on couples with two or more prior pregnancy losses. For example, the frequency of both monosomy and trisomy in all chromosomes was fairly equally distributed with the aneuploidy rate ranging from 3.1 to 5.8%.
This is in stark contrast to the aneuploidy rates that are seen in the miscarriage tissue in which abnormalities in chromosomes 15, 16, 21, and 22 account for 60% of the abnormalities that are seen. This strongly suggests that many of the pregnancy losses that we term “biochemical” are due to aneuploidies in some of the larger chromosomes and that there is such a disparity in genetic material that is present in the embryo that growth cannot continue more than a few days before the pregnancy fails.
To see a fertility specialist with many decades of experience treating patients who have had multiple miscarriages and / or repeated pregnancy loss, make an appointment at one of InVia’s four Chicago area fertility clinics.
[hs_action id="4078"]

Dr. Karande is Board Certified in the specialty of Obstetrics and Gynecology as well as the subspecialty of Reproductive Endocrinology and Infertility. He is a Fellow of the American College of Obstetricians and Gynecologists and Member of the American Society for Reproductive Medicine.
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists


Comments