Tubal factor is a major cause of female infertility. Evaluation of the fallopian tubes is routinely done as part of an infertility work up. Several techniques have been used to evaluate the fallopian tubes. These include X-ray (hysterosalpingogram, HSG); ultrasound (hystero-contrast-sonography (HyCoSy); three-dimensional Doppler tubal flow measurements); and laparoscopy. HSG remains the most commonly used technique for evaluating the tubes. The question is, what can be done if the tubes are blocked? The answer (in selected cases) is tubal catheterization (TC). At InVia Fertility Specialists, we will often do a HSG and immediately proceed with TC if there is tubal blockage. TC is less invasive and more cost-effective than other options such as laparoscopy, tubal microsurgery or in vitro fertilization (IVF). The best part is that it is simple and it works!
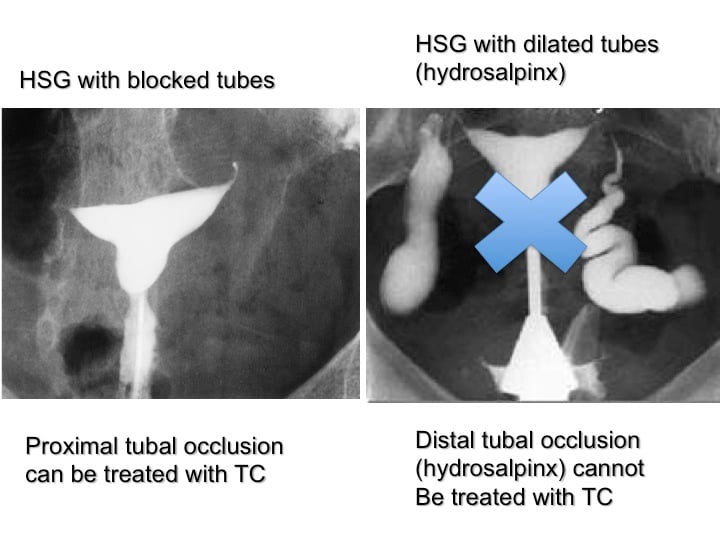
TC can be done when there is proximal tubal occlusion (PTO; the tubes are blocked at the uterine end). Patients with distal tubal occlusion (the tubes are blocked at the fimbrial end) often have hydrosalpinx and are NOT candidates for TC. TC is not indicated when there has been a tubal ligation. In patients with salpingitis isthmica nodosa; TC should be deferred as IVF is the treatment of choice in these patients.
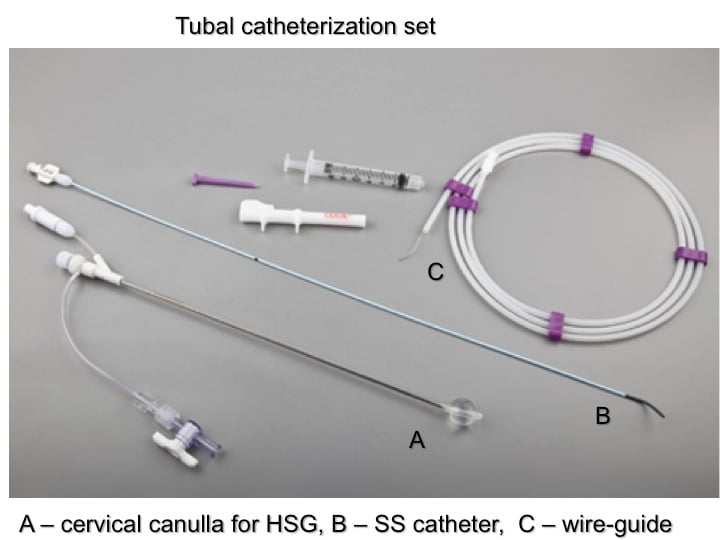
TC involves the use of specially designed coaxial catheter systems. There is the uterine access balloon catheter (see above; A) that is used for performing HSG. It has a balloon at its tip, which is inflated with air to hold it in place in the cervix or lower uterine cavity. It also has a central channel, which allows introduction of other catheters. The selective salpingography (SS) catheter (see above; B) can be inserted through the central channel of the cervical canulla. It has a curved tip and can be manipulated into the tubal ostia (opening). The third component is a wire-guide (see above; C). This has a special coating that makes it slippery and easy to manipulate into the tubal lumen.
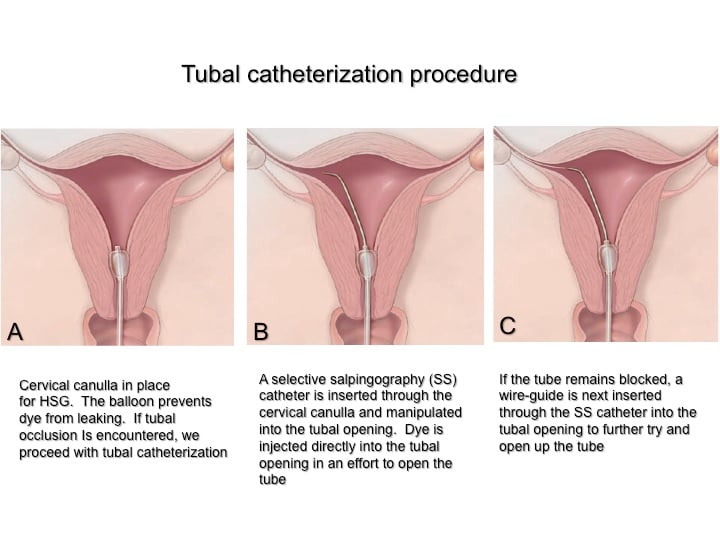
TC involves the use of specially designed coaxial catheter systems. The first step (see above; A) is to do a HSG with the uterine access balloon catheter in place and confirm the diagnosis of PTO. A SS catheter is then inserted coaxially through the cervical canulla and manipulated into the tubal ostia (see above; B). Dye can then be injected directly into the tubal opening and will often open up the blocked tube. Should this fail; the wire-guide is inserted through the central channel of the SS catheter into the tubal ostia (see above; C). It is then advanced past the occluded portion of the tube into the distal tubal lumen and is moved in a to and fro manner to further open up the tube. This is similar to what a plumber does to open up a blocked pipe!
The discomfort experienced during TC is not much different than a HSG. We pre-treat patients with Ibuprofen 800 mg and give a local anesthetic (paracervical block) to further reduce any discomfort.
Images from an actual procedure and success rates will be presented in a subsequent blog.
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists

