I have previously discussed the impact of the thyroid gland on female reproduction. Hypothyroidism (“low” thyroid) is fairly common and according to the National Health and Nutrition Examination Survey (NHANES) affects 0.3% of women. It is diagnosed by an elevated thyroid stimulating hormone (TSH) level and low free thyroxine (FT4) level. Subclinical hypothyroidism is when the patient is completely asymptomatic but the thyroid stimulating hormone level is elevated (FT4 is normal). According to NHANES, 4.3% of women will have subclinical hypothyroidism. In a recent blog, we discussed the impact of uncorrected subclinical hypothyroidism on IVF pregnancy rates. In this blog, we will be discussing clinical management of TSH levels.
Measurement of serum TSH is the primary screening test for thyroid dysfunction. At InVia Fertility Specialists, we will usually measure TSH levels in all of our fertility patients.
TSH levels do vary during the day by up to 50% of mean values. Values tend to be lowest in the late afternoon and highest around the hour of sleep. Keeping this in mind, variations of serum TSH values within the normal range of up to 40 – 50% do not necessarily reflect a change in thyroid status.
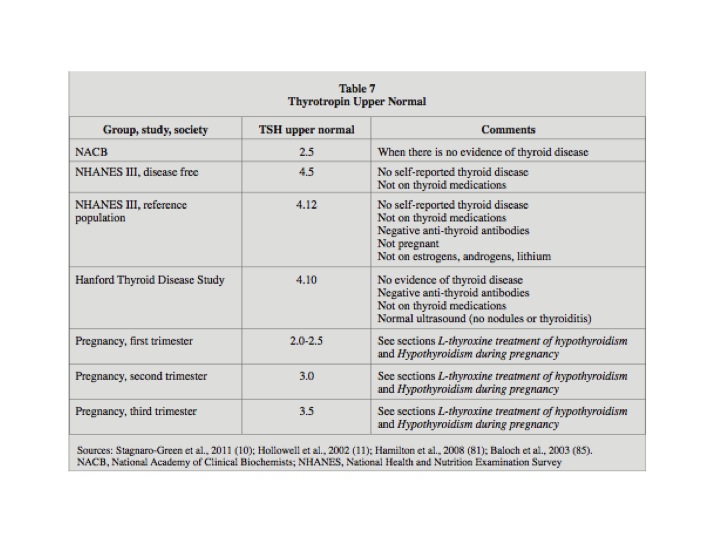
What is a normal TSH level? According to the American Thyroid Association (ATA) and American Association of Clinical Endocrinologists (AACE) in women of childbearing age planning to get pregnant (and in the first trimester of pregnancy) the TSH level should be maintained below 2.5 mIU/mL. The “normal” level may also be different in other clinical situations as shown in the table below.
What is the treatment of hypothyroidism? The treatment is with thyroid hormone pills (L-thyroxine, Synthroid, levothyroxine). The daily dose of L-thyroxine is dependent on age, sex and body size. The usual dose in is 1.6 mg/kg of L-thyroxine daily. Patients with central hypothyroidism (thyroid gland is removed (total thyroidectomy) and/or after radioiodine therapy) will require higher doses of L-thyroxine.
What about subclinical hypothyroidism? These patients do not require full replacement doses. Doses of 25 – 75 mg are usually sufficient. Generally, the dose varies based on the TSH level. L-thyroxine 25 mg is used when the TSH level is between 4 – 8 mIU/mL; 50 mg for TSH 8 – 12 mIU/mL and 75mg for TSH > 12 mIU/mL. After the first two months; only minimal further adjustments are required to normalize TSH levels.
L-thyroxine is best absorbed on an empty stomach and should be taken 30 to 60 minutes prior to eating breakfast or at bedtime 4 hours after the last meal. L-thyroxine can be stored at room temperature (68 – 77 degrees F or 15 – 30 degrees C).
Dose adjustments are to be made 4 – 8 weeks after the starting dose. The dose can be increased by 12.5 to 25 mg/d initially, but even smaller changes may be necessary to achieve goal TSH levels. In pregnancy thyroid hormone requirements are increased, then revert back to baseline after delivery.
In patients with central hypothyroidism; free T4 levels (and not TSH levels) should guide therapy.
Once an adequate replacement dosage has been determined, repeat TSH testing at 6-month and then 12-month intervals are generally considered appropriate.
In early pregnancy, there is a rise in serum total T4 levels. There are studies suggesting that this rise in serum T4 levels is essential for the proper intellectual development of the baby. Desiccated thyroid and L-thyroxine combinations (e.g. Armor thyroid) cause lowering of serum T4 levels and should NOT be used during pregnancy. In fact pregnant patients (or those trying to conceive) on Armor thyroid should be switched to L-thyroxine.
Infertility Infertility treatment InVia Fertility Specialists Early pregnancy Top 10
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists

