The goal of a successful embryo transfer (ET) is to deliver the embryo(s) in the uterus without damaging them. Historically, embryo transfer ET was carried out with the “clinical touch” technique. This involved advancing the transfer catheter until contact was made with the top of the uterine cavity (uterine fundus), then withdrawing the catheter 5 – 10 mm before expelling the embryos. With the use of ultrasound, it became apparent that with this “blind’ technique, the catheter was poorly positioned 20% of the time. Over the past two decades, “clinical touch” technique has been largely replaced by ultrasound guidance.
Here are some interesting facts about ultrasound-guided ET.
Ultrasound guidance ensures correct location of the catheter in the uterine cavity. A group from Australia (Woolcott and Stanger,1997) showed that with “clinical touch” alone, the catheter was below the uterine lining (sub-endometrial) 24.7%, touching the fundus 17.4% and in the opening of the fallopian tube 7.4% of the time!
When the catheter touches the uterine fundus, it causes uterine contractions, which may result in the embryos being expelled. Also the resultant trauma (blood seen in the catheter tip after the ET) results in lower pregnancy rates. Touching the fundus can easily be avoided with ultrasound.
One can be sure the catheter is beyond the internal os in cases of an elongated cervical canal. Some patients (especially those who have had fibroids removed) will have longer than usual cervical canals. With “clinical touch” it is not always possible to ensure that the catheter tip is beyond the internal os of the cervix and has reached the uterine cavity.
We have had several patients with a previous C-Section that have a defect in the lower uterine segment at the site of the C-section incision. The ET catheter can get hung up or misdirected in this “pocket” with a resultant negative pregnancy test.
Direct visualization of the catheter at the uterocervical angle can facilitate its insertion. When the angle is clearly visualized, the physician can place an appropriate curve on the catheter, which can help negotiate the canal especially when the uterus has a severe angle (severely ante flexed or retroflexed). This helps increase the chances of the transfer being “easy” with a resultant increased pregnancy rate.

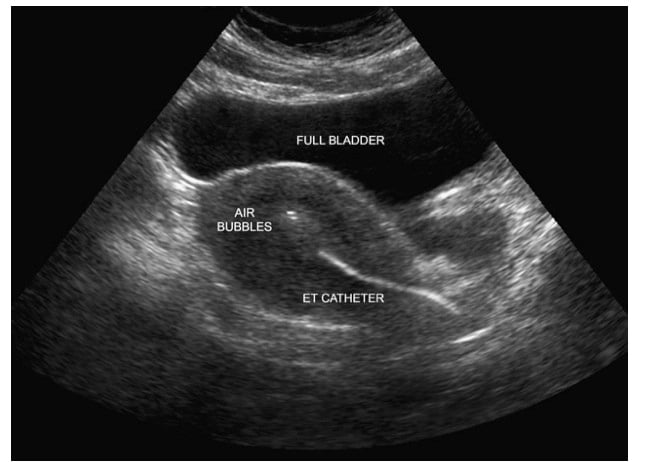
The full bladder acts as an “ultrasonic window” and facilitates visualization with a transabdominal probe. It also helps to straighten the uterocervical angle and facilitate entry of the catheter, particularly for the strongly anteverted uterus.
Patients love visualizing the final step where they get to see the “flash” from the air and fluid surrounding the embryo(s). It is really cool to visualize the moment you get (theoretically) pregnant!
One disadvantage with ultrasound is the inconvenience patients experience when they have to wait with a full bladder. We are well aware that it is not fun to wait with a full bladder. We do try our very best to do the ET on time!
The most important fact is that pregnancy rates are higher with ultrasound-guided ET! This has been confirmed by two meta-analyses and by a 2010 Cochrane review.
Some programs, however, have reported excellent pregnancy rates with the “clinical touch” technique (they usually perform a “trial” transfer to map the cervical canal and the embryos are transferred without the catheter tip touching the uterine fundus) and for them it is okay to continue doing whatever works for them.
Infertility Infertility treatment IVF InVia Fertility Specialists Top 10
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists

