Endometriosis is a condition where the lining of the uterus (endometrial-like glands and stroma) is present outside the uterus. These implants are sensitive to hormonal changes and result in chronic inflammation and changes in the immune system, resulting in a wide range of symptoms.
Endometriosis is common—in fact, a 2015 study estimates that 6.5 million women in the U.S. between the ages of 15-44 are likely to have it, which is around 11% of women. Endometriosis can also take a long time to diagnose. Studies show that it can take anywhere from four to 11 years! In this post, I will give an overview of what the most common symptoms of endometriosis are, and why those symptoms can result in such a long time to diagnosis.
Many patients with endometriosis will have no symptoms. However, the most common clinical presentations of endometriosis are infertility, painful periods and pelvic masses.
Patients often report pain with onset of menses that gets progressively worse over a period of time. In the initial stages, pain relief is achieved with over-the-counter pain pills (e.g., Motrin or Aleve). The pain can sometimes increase to a point where these pain pills do not work, resulting in disruption to daily activities and an overall decrease in the quality of life.
Another common symptom is pain with intercourse. This pain is usually deep inside the vagina. Sometimes couples can work out which positions to avoid.
The table below shows the overlap of symptoms between endometriosis and other causes of pain. As you can see, depending on how it is affecting the patient’s body, endometriosis can look like many other things, including irritable bowel syndrome or a bladder infection.
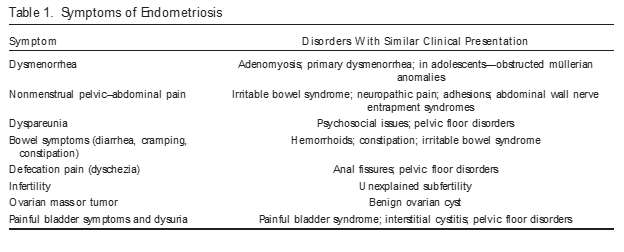
Table source: https://pubmed.ncbi.nlm.nih.gov/29420391/
This overlap of symptoms is part of the reason why the average age at diagnosis is approximately 28 years, and why there often is a delay of seven to eight years on average from the onset of symptoms to a definitive diagnosis of endometriosis.
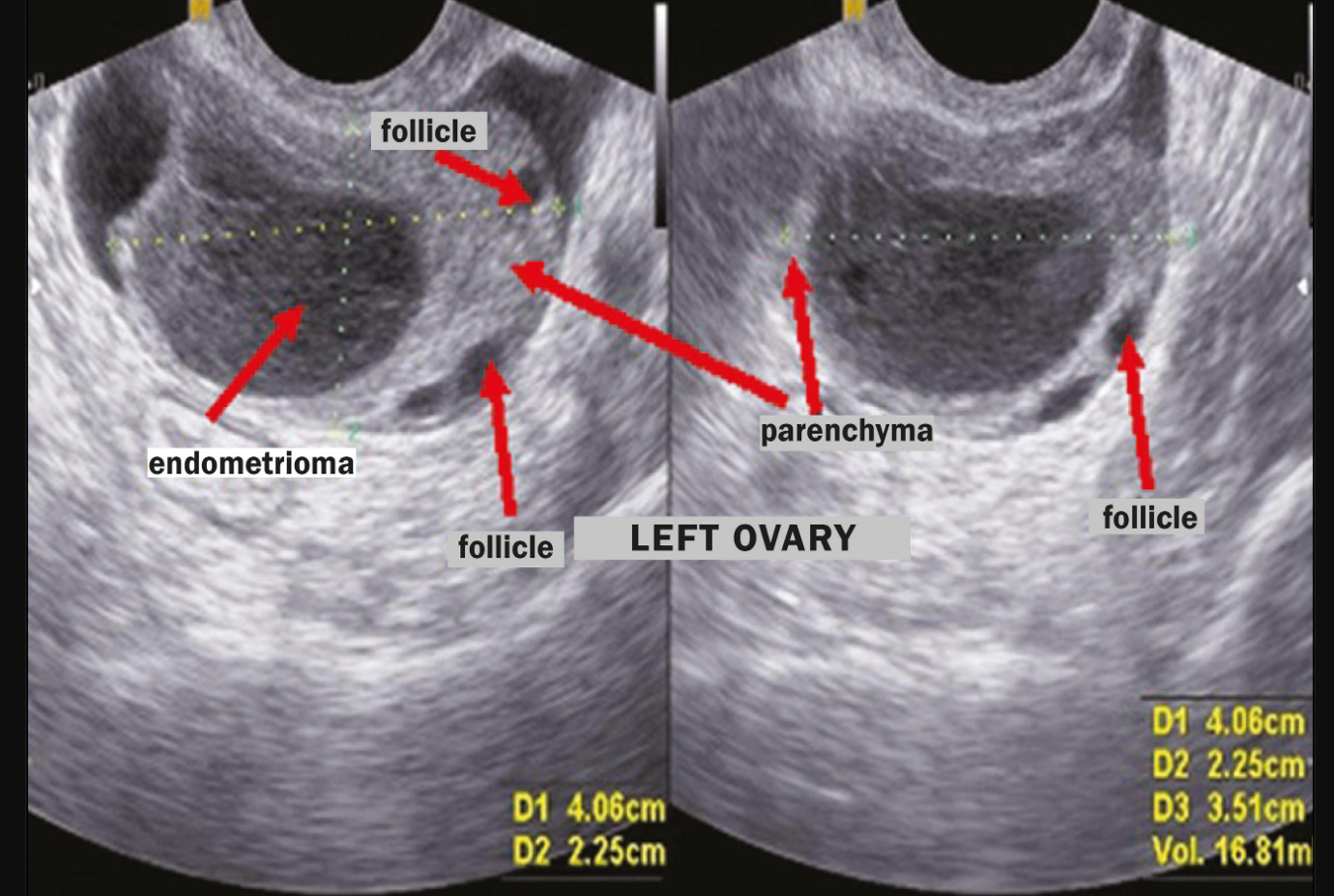
A pelvic examination can be useful for diagnosing endometriosis. The presence of tender areas (nodules) on digital examination or the presence of a pelvic mass are suspicious of a diagnosis of endometriosis. A pelvic ultrasound with a vaginal probe is another excellent diagnostic tool. Ovarian cysts caused by endometriosis (endometrioma) can be seen with ultrasound.
However, endometrial adhesions (“sticky” bands of endometrial tissue) may be difficult to diagnose using digital examination or ultrasound. Therefore, a surgical procedure (laparoscopy) remains the gold standard for diagnosing endometriosis. An experienced surgeon can diagnose and remove endometriosis during the same surgery.
In an effort to reduce time to diagnosis and the need for surgical intervention, researchers are at work trying to develop non-invasive tests for endometriosis.
One non-surgical test for endometriosis which has emerged on the market is ReceptivaDx™. This is a new test for endometrial receptivity that provides enhanced screening for all stages of endometriosis and other conditions that interfere with implantation.
According to the company's website, ReceptivaDx has high sensitivity and specificity (96%) and is especially useful for women with unexplained IVF failure or infertility. It identifies BCL6, a gene repressor biomarker that is present in the setting of inflammation. BCL6 is dramatically over-expressed in women with endometriosis, making it a likely candidate for the cause of progesterone resistance that contributes to implantation problems.
Progesterone is required for normal pregnancy, so a protein that interferes with progesterone action would explain much about the problems encountered in women with endometriosis. Studies have shown that women with elevated BCL6 results are five times less likely to succeed in IVF or subsequent transfer attempts. A negative BCL6 result provides reassurance to patients that endometriosis is not of concern.
If endometriosis is suspected, it can be treated by your physician. Current treatments include hormone therapy or laparoscopy. Patients can resume pregnancy attempts shortly after treatment with renewed confidence.
There are still many challenges facing endometriosis patients as they try to build their families, but treatment is possible. If you are in the Chicago area, InVia Fertility Specialists is here for you.
We have four convenient locations around Chicago where you can work with our board-certified team of fertility doctors, all of whom are experienced in successful treatment of endometriosis and the fertility problems it can cause.
You can click below to make an appointment online. We will be happy to answer your questions and help you find your pathway to pregnancy!

Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists

