Endometriosis
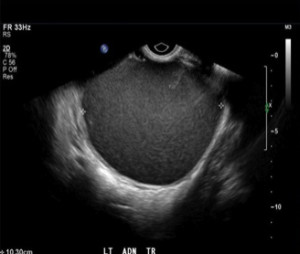
Endometriosis is a condition where the uterine lining (endometrium – shown at right via ultrasound) ) is present outside the uterine cavity. An
endometrioma is a blood-filled "chocolate" cyst that can occur when endometriosis tissue develops in the ovary.
By definition, a patient with endometrioma has “severe” or Stage IV endometriosis. These patients can be severely symptomatic (painful periods that are getting progressively worse, pain with intercourse) and infertile.
The treatment of ovarian endometriomas remains controversial. Initial studies tried to demonstrate a link between endometriomas and infertility, and increased fertility after endometrioma surgery. With the development of in vitro fertilization (IVF), doubts were raised about the utility of surgery for fertility purposes in women with endometrioma. Some investigators even suggested that fertility may be reduced as a result of traumatic surgery, as it removes not only the endometrioma but also healthy ovarian cortex.
Should we perform surgery for endometriomas? Is there a best technique? Researchers from the Universite Catholoque de Louvain, Brussels, Belgium and the Nagasaki University School of Medicine, Nagasaki, Japan addressed these very questions (Jadoul et al. Fertil Steril 2012;98:556-63).
Arguments in Favor of Surgery for Endometrioma
- Most women with endometriosis complain of menstrual or extramenstrual pain. It is widely accepted that these symptoms will be greatly improved by surgery.
- Several studies have shown increased fertility after surgical treatment of endometriomas. Pregnancy rates of approximately 50% have been shown in the first year after surgical removal of endometriomas.
- Third, a recent review of the literature by Nyhøj et al. showed a possible link between endometriosis and ovarian cancer. This increased risk factor is an argument for surgery, especially in patients over 45 years of age with ovarian endometriomas, and particularly if the endometriomas are recurrent, which is probably indicative of a more aggressive form of the disease.
- In cases of IVF in women with endometriomas, one should take into account the possible difficulty of accessing the follicles and the risk of pelvic infection after inadvertent drainage of endometriomas at the time of egg retrieval. Drainage of an endometrioma at the time of egg retrieval may not only increase the risk of infection but also affect the quality of eggs contaminated by the ‘‘chocolate’’ fluid.
Arguments Against Surgery for Endometrioma
- Surgery may actually reduce chances of conception by decreasing ovarian reserve and sometimes result in premature ovarian failure. This is especially so when the cyst wall is surgically “stripped” from the ovary. This procedure (ovarian cystectomy) can result in removal of normal ovarian cortex in 6% of cases, and normal ovarian tissue in more than 50% of cases. In cases where the cyst wall is burnt (electrocoagulation) there will be damage to underlying normal ovarian tissue.
- IVF outcomes after surgical treatment of endometriomas show no increase in pregnancy rates after surgery. In fact, there may be a decrease in pregnancy and implantation rates after surgery. The number of mature eggs retrieved is also decreased after surgery. Almost all studies comparing the number of retrieved and mature eggs between operated ovaries and contralateral nonoperated ovaries show a statistically significant increase in favor of nonoperated ovaries.
- Surgery may precipitate premature ovarian failure and diminish ovarian reserve. AMH levels will often decrease after surgery.
So What Should We Do?
The authors opine that several facts should be considered before deciding to operate. These include the patient's age, her symptoms, whether she wants to conceive soon, previous surgery, other indications for IVF and endometrioma size.
In patients with no other infertility factor that wish to conceive soon, surgery may be indicated.
Repeat surgery is generally to be avoided and IVF may be the better option.
The authors also suggest that endometrioma larger than 3 cm should be removed before IVF.
Read more about endometrioma surgical techniques in this blog.