
 In a previous blog we discussed the expected ultrasound findings in a normal intrauterine pregnancy. Variations from the expected pattern of development are worrisome or, if major, definitive for early pregnancy failure or miscarriage. These were discussed in a recent review article by Doubilet et al. (N Engl J Med 2013;369:1443-51). Here is a summary:
In a previous blog we discussed the expected ultrasound findings in a normal intrauterine pregnancy. Variations from the expected pattern of development are worrisome or, if major, definitive for early pregnancy failure or miscarriage. These were discussed in a recent review article by Doubilet et al. (N Engl J Med 2013;369:1443-51). Here is a summary:
The criteria most often used to diagnose pregnancy failure are the absence of cardiac activity by the time the embryo has reached a certain length (crown–rump length), the absence of a visible embryo by the time the gestational sac has grown to a certain size (mean sac diameter), and the absence of a visible embryo by a certain point in time.
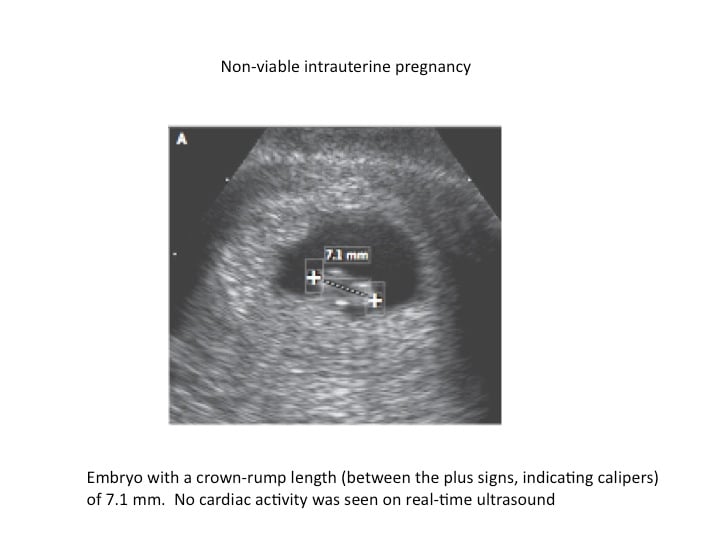
A crown–rump length of 5 mm was widely recommended as a positivity criterion for diagnosing failed pregnancy when no cardiac activity is seen. Recent studies have shown that a 5-6 mm cutoff can result in a false positive diagnosis of pregnancy failure. It is now recommended that we use a 7 mm (rather than 5 mm) cut-off for diagnosing failed pregnancy. Thus if the crown-rump length is 7 mm and there is no heart beat visible, it is suspicious for a failed pregnancy.
It is prudent to use a cutoff of 25 mm (rather than 16 mm) for the mean sac diameter with no visible embryo in diagnosing failed pregnancy (see figure above). This would yield a specificity and positive predictive value of 100% (or as close to 100% as can be determined). When the mean sac diameter is 16 to 24 mm, the lack of an embryo is suspicious for, though not diagnostic of, failed pregnancy
 Not all failed pregnancies ever develop a 7-mm embryo or a 25-mm gestational sac, so it is important to have other criteria for diagnosing pregnancy failure. The most useful of such criteria involve non visualization of an embryo by a certain point in time. An alternative approach to predicting pregnancy failure, based on subnormal growth of the gestational sac and embryo, has been shown to be unreliable. Non visualization of an embryo with a heart- beat by 6 weeks after the last menstrual period is suspicious for failed pregnancy, but dating of the last menstrual period (in a pregnancy conceived without medical assistance) is too unreliable for definitive diagnosis of pregnancy failure.
Not all failed pregnancies ever develop a 7-mm embryo or a 25-mm gestational sac, so it is important to have other criteria for diagnosing pregnancy failure. The most useful of such criteria involve non visualization of an embryo by a certain point in time. An alternative approach to predicting pregnancy failure, based on subnormal growth of the gestational sac and embryo, has been shown to be unreliable. Non visualization of an embryo with a heart- beat by 6 weeks after the last menstrual period is suspicious for failed pregnancy, but dating of the last menstrual period (in a pregnancy conceived without medical assistance) is too unreliable for definitive diagnosis of pregnancy failure.
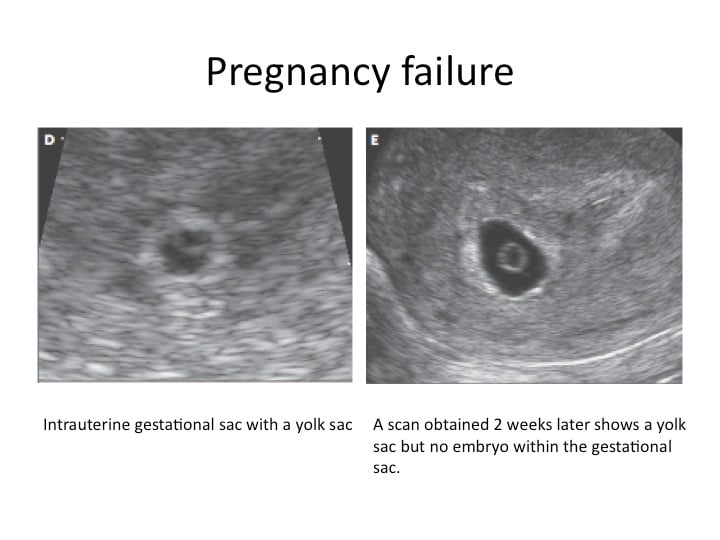
The timing of events in early pregnancy — gestational sac at 5 weeks, yolk sac at 5 ½ weeks, and embryo with heartbeat at 6 weeks — is accurate and reproducible, with a variation of about ± ½ week; this consistency explains the time-related criteria for pregnancy failure. For example, if the initial ultrasonogram shows a gestational sac with a yolk sac and a follow-up scan obtained at least 11 days later does not show an embryo with cardiac activity, the diagnosis of failed pregnancy is established.
According to the Society of Radiologists in Ultrasound Multispecialty Consensus Conference on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy, October 2012; the following are guidelines for Transvaginal Ultrasonographic diagnosis of Pregnancy Failure in a Woman with an Intrauterine Pregnancy of Uncertain Viability.
When there are findings suspicious for pregnancy failure, follow-up ultrasonography at 7 to 10 days to assess the pregnancy for viability is generally appropriate. Treatments for early miscarriage are discussed here.
To see a fertility specialist who is a board-certified physician with high success rates, make an appointment at one of InVia’s four Chicago area fertility clinics.
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists

