Approximately one in every seven couples in the United States has problems conceiving. Male infertility accounts for half of these cases. Even with these statistics infertility evaluations have traditionally focused on women, because women tend to seek gynecological care and because men are reluctant to seek advice from a physician. A semen analysis is the first step in evaluation of the male. Question is, what can be done if the test results are abnormal?
Male infertility has many causes--from hormonal imbalances, to physical problems, to psychological and/or behavioral problems. A small percentage of male infertility is indeed caused by hormonal problems. Hormonal problems include male hypogonadism (low testosterone levels), testicular failure and others (elevated prolactin levels).
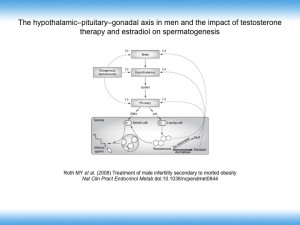 The hypothalamus-pituitary endocrine system regulates the hormones that enable the testes to produce sperm (see figure). Follicle stimulating hormone (FSH) stimulates the Sertoli cells in the testis to produce sperm and luteinizing hormone (LH) stimulates the Leydig cells in the testis to produce testosterone. The pituitary can fail to produce enough FSH and LH with a resultant drop in sperm and testosterone production (hypogonadism). In this situation, the testosterone level will be low (< 300 ng/dl).
The hypothalamus-pituitary endocrine system regulates the hormones that enable the testes to produce sperm (see figure). Follicle stimulating hormone (FSH) stimulates the Sertoli cells in the testis to produce sperm and luteinizing hormone (LH) stimulates the Leydig cells in the testis to produce testosterone. The pituitary can fail to produce enough FSH and LH with a resultant drop in sperm and testosterone production (hypogonadism). In this situation, the testosterone level will be low (< 300 ng/dl).
Increases in the amount of testosterone converted to estrogen under the action of the enzyme aromatase may also contribute to hypogonadism (see figure). Peripheral fat cell are hormonally active and contain the enzyme aromatase. In obese patients, increased aromatase activity is thought to result in increased estradiol production (levels > 54 pg/ml are considered elevated). The increased estradiol level inhibits FSH and LH secretion from the pituitary, which results in reduced FSH and LH stimulation of the Sertoli and Leydig cells in the testes and a reduction in testosterone synthesis and sperm production. Administration of exogenous testosterone effectively raises serum testosterone levels. If fertility is desired administration of testosterone is, however, counterproductive because it provides negative feedback to the pituitary and causes inhibition of LH and FSH secretion. Decreased LH and FSH stimulation of the testes further inhibits spermatogenesis.
Clinically, male hypogonadism may be characterized by loss of vitality, fatigue, loss of libido, erectile dysfunction, sleepiness, depression and poor concentration. Hypogonadal ageing men also gain fat mass and lose bone mass, muscle mass and strength.
If the problem is with the testis (testicular failure), the pituitary gland will release more FSH and LH in an attempt to stimulate the testes. Testicular failure can therefore be diagnosed if the FSH/LH levels are elevated. Clinically, in this situation, the testis can be small (reduced testicular volume). Often, the testosterone levels are normal.
Another hormone that plays a role in male factor infertility is prolactin. Elevated prolactin (a hormone usually associated with nursing mothers) is found in 10 to 40 percent of infertile males (normal range in males 2.1-17.7ng/ml). Mild elevation of prolactin levels produces no symptoms, but higher levels of the hormone reduces sperm production, reduces libido and may cause impotence.
The majority of testosterone is bound to proteins (sex hormone binding globulin (SHBG) and albumin) and is not available for the tissues. Free testosterone is the fraction that is not bound to protein and is the active form of the hormone. We therefore measure both total as well as free testosterone levels. Testosterone levels fluctuate during the day and are highest in the morning just after waking up. We therefore like to measure testosterone before 11 am when the level is highest.
When the testosterone level is low, the logical approach might be to give supplemental testosterone. In fact, that is the wrong thing to do! Prolonged use of testosterone can have the opposite effect, compromising sperm counts, lowering motility and even poor morphology (see figure).
Hormone therapy can be very effective when the right medication is given in the correct dose to men with low hormone levels. The most commonly prescribed male fertility medication is clomiphene citrate or Clomid. Yes this is the same drug that many female fertility patients take! Clomiphene citrate works essentially the same way in both women and men; in women, it binds to receptors in the brain (specifically the hypothalamus and the pituitary gland) to increase the production of follicle stimulating hormone (FSH) (normal range 1.4-18.0 mIU/ml) and luteinizing hormone (LH) normal range 1.5-9.3 mlIU/ml). These hormones act on the ovarian follicles to induce egg development and ovulation. In men, the increase in FSH leads to an increase in sperm production, whereas the increase in LH leads to an increase in testosterone production.
The total testosterone level needs to be above 300 ng/dl. If lower than 300 ng/dl, clomiphene citrate 25 mg orally daily for a minimum of 3 – 4 months is prescribed. Immediate improvement is not seen since new sperm production takes 60 – 72 days.
Aromatase inhibitors such as anostrozole (Arimidex) are useful when estradiol levels are elevated in mean (normal range in males less than 54 pg/ml). In these patients, testosterone is NOT indicated as it will worsen the situation (see figure above). Weight loss will help reduce fat cells, which are the primary source of the enzyme aromatase.
Elevated prolactin levels are treated with the drug bromocriptine (Parlodel). In some of these men, especially when the prolactin levels are really high, a MRI of the pituitary gland is necessary to rule out a pituitary adenoma (tumor).
If the case of male factor infertility is testicular failure, hormonal treatment is usually not effective. These patients will benefit from assisted reproductive technologies (intrauterine insemination, intracytoplasmic sperm injection (ICSI), testicular sperm aspiration).
Lifestyle improvement can help. These include quitting smoking, losing excess weight, limited use of alcohol, not using recreational drugs like marijuana and anabolic steroids. Tight underwear and steam baths increase scrotal temperature with a resultant decrease in sperm production.
Varicocele surgery is controversial. Recent publications have shown that microsurgical varicocele repair is the preferred technique.
Anti-oxidants and other dietary supplements can be improve success rates and have been discussed in other blogs.
Infertility treatment IVF Male factor InVia Fertility Specialists
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists

