Tubal pregnancy is possible regardless of how you get pregnant. But there are some unique aspects to tubal pregnancy that pertain to cases in which IVF is used. Here are ten interesting facts about IVF and tubal pregnancy:
A tubal pregnancy (also called an ectopic pregnancy) is a pregnancy that is implanted outside the uterus. During in vitro fertilization (IVF) embryo(s) are transferred into the uterus. However, subsequent uterine contractions can squeeze the embryo(s) into the tube where they can implant and result in a tubal pregnancy.
The first ever IVF pregnancy was a tubal pregnancy! With IVF, since more than one embryo may be transferred, it's possible to get an unusual combination of tubal and intrauterine pregnancies, e.g. one in the uterus and one in the tube, etc.
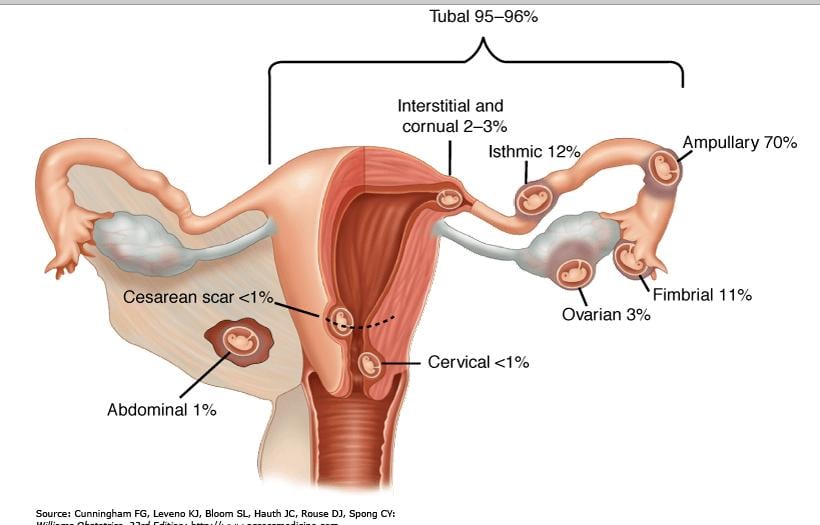
The incidence of tubal pregnancy after IVF is relatively high at 2 – 5%. The reason for this increase remains unclear. There is an increased chance of getting an isthmic or a corneal tubal pregnancy with IVF.
These days, most fertility centers are doing embryo transfers under ultrasound guidance. This ensures proper placement of the embryos in the uterine cavity. Surprisingly, ultrasound guidance has not reduced the incidence of tubal pregnancy with IVF.
Despite scant evidence, it has been suggested that high placement of embryos in the uterine cavity, higher volumes of transfer media and rapid plunging of the syringe attached to the embryo transfer catheter and transfer of may increase incidence of tubal pregnancy.
Risk of tubal pregnancy increases with the number of embryos transferred during IVF treatment.
Women undergoing IVF because of tubal factor infertility (previous infection, surgery or tubal pregnancy) are at higher risk for tubal pregnancy than women undergoing IVF for male factor infertility.
It is also proposed that an "embryo factor" may be present. This involves the cell adhesion protein, E-cadherin, which is essential for blastocyst formation prior to implantation. In IVF, the embryos are exposed to a different growth factor and cytokine milieu during in vitro culture compared with naturally conceived embryos. This results in a difference in localization if E-cadherin making such embryos unable to implant within the uterus and instead migrate into the Fallopian tube and attach to the tubal epithelium.
With early diagnosis, it is now often possible to treat tubal pregnancy medically with the drug Methotrexate and thus avoid surgery. In IVF patients, one should be careful to rule out a concurrent intrauterine pregnancy — one embryo implanted in the uterus and the other in the tube, or both implanted in the tube. If this is the case, surgery is needed to treat the tubal pregnancy.
Patients with a history of one tubal pregnancy have a 60% chance of a spontaneous intrauterine pregnancy. However, in patients with a history of two tubal pregnancies, the best option is IVF.
To see a fertility specialist who is a board-certified physician with high success rates, make an appointment at one of InVia’s four Chicago area fertility clinics.
Entire Website © 2003 - 2020
Karande and Associates d/b/a InVia
Fertility Specialists

